Under constant illumination, pupil diameter is not static but exhibits continuous, rhythmic fluctuations characterized by alternating constriction and dilation. These oscillations typically have an amplitude of up to 0.5 mm (approximately 4% of the iris diameter) and a frequency ranging from 0.1 to 2 cycles per second. Such spontaneous oscillatory activity is referred to as hippus. The amplitude of hippus diminishes under bright illumination and is greatest when the pupil is of intermediate size, a state in which the iris demonstrates maximal mobility.
An increase in oscillation amplitude exceeding 1 mm (more than 8% of the iris diameter) may be observed in various vascular, inflammatory, degenerative, and traumatic disorders of the nervous system and is often considered an early clinical indicator of multiple sclerosis. In contrast, a marked reduction or absence of spontaneous pupillary oscillations—resulting in so-called “stone pupils”—is associated with severe neurogenic, psychiatric, visceral, and infectious conditions, as well as terminal states such as syncope, shock, sepsis, and coma.
The phenomenon known as “jumping pupils” describes sudden, nearly instantaneous pupillary dilations that alternate unpredictably between the eyes and occur independently of external stimuli. Despite these abrupt changes, other pupillary responses—including reactions to light, accommodation, convergence, and pharmacologic agents—remain preserved. This rare finding has been reported in association with conditions such as neurasthenia, epilepsy, myelitis, progressive paralysis, and Graves’ disease.
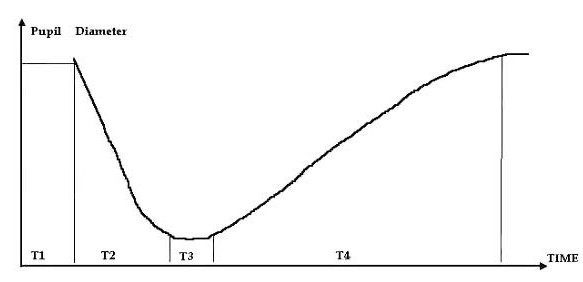
Pupillary light reflexes are of particular diagnostic importance and include both direct and consensual responses. The direct light reflex refers to constriction of the illuminated pupil, whereas the consensual reflex describes simultaneous constriction of the contralateral pupil. The temporal characteristics of these responses, collectively termed the pupillary cycle, comprise four parameters: the latency to constriction, the duration of constriction, the latency to redilation, and the duration of redilation.
Abnormal Pupillary Reactions
Anatomical Forms of Pupillary Immobility
Several forms of abnormal pupillary reactions, many of which constitute key elements of classic neuropathological syndromes, are outlined below.
Amaurotic Pupillary Immobility
This condition is characterized by the absence of both direct and consensual light reflexes in one or both pupils, while accommodation and eyelid-closure responses may remain intact. Bilateral amaurotic immobility results from damage to both retinas or to the optic tracts proximal to the primary visual centers, leading to bilateral blindness and marked pupillary dilation. In unilateral lesions of the retina or optic tract, the affected eye fails to respond to light, whereas the contralateral eye exhibits preserved direct and consensual reactions. The pupil of the affected eye is typically more dilated. Amaurotic immobility most commonly follows optic neuritis or optic nerve atrophy.
Hemianoptic Pupillary Immobility
Hemianoptic immobility arises from lesions of the optic tract proximal to the lateral geniculate body. Illumination of the non-functioning retinal hemifield fails to elicit either direct or consensual pupillary responses, while stimulation of intact retinal regions produces normal reactions. Lesions located distal to the divergence of the pupillary light reflex fibers do not result in hemianoptic immobility. This phenomenon reflects disruption at the anatomical level where optic nerve fibers and pupillary reflex pathways converge.
Absolute Pupillary Immobility
Absolute immobility is defined by a complete absence of pupillary responses to both light and accommodation. It is typically unilateral and accompanied by mydriasis. This condition results from damage to the oculomotor parasympathetic pathways, extending from the Edinger–Westphal nucleus to the sphincter pupillae muscle.
Reflex Forms of Pupillary Immobility
Argyll–Robertson Syndrome
This reflex pupillary disorder may be unilateral or bilateral and is characterized by loss of both direct and consensual light reflexes, with preserved or exaggerated accommodation-convergence responses and associated miosis. Structural iris changes may include smoothing of surface relief, partial depigmentation, and sectoral atrophy. Early in the disease course, light responses may be delayed and diminished before disappearing entirely. The condition may exhibit periods of remission and exacerbation. While classically associated with neurosyphilis, Argyll–Robertson–like phenomena may also occur in intracranial tumors, encephalitis, cranio-cerebral trauma, multiple sclerosis, and chronic alcoholism.
Functional and Neurogenic Pupillary Abnormalities
Paradoxical Pupillary Reaction
This abnormality is characterized by pupillary dilation in response to light and constriction in darkness. It is attributed to disruption of cortical inhibitory mechanisms and may be observed in lesions of the upper cervical sympathetic ganglia, oculomotor nerve paralysis, or intracranial hemorrhage.
Myotonic Pupillary Reaction
Myotonic reactions involve delayed and prolonged pupillary constriction during accommodation and convergence, with diminished or absent responses upon repeated fixation of distant objects. This pattern is commonly observed in multiple sclerosis, diabetes mellitus, intracranial tumors, and traumatic brain injury.
Neurotonic Pupillary Reaction
Neurotonic reactions are marked by delayed constriction in response to illumination, followed by slow redilation after cessation of the stimulus. This pattern is associated with autonomic dysregulation and is observed in vegetative neurosis, chronic alcoholism, heavy tobacco use, and progressive paralysis.
Pupillotonia (Adie’s Syndrome)
Pupillotonia is characterized by a weak or absent light reflex, slow and prolonged accommodation responses, and delayed redilation after extended periods of darkness. The condition is frequently unilateral, often accompanied by anisocoria, and associated with hypersensitivity to cholinergic agents.
Intravegetative Pupillary Stupor Syndrome
This syndrome is defined by a prolonged latent phase preceding pupillary dilation, producing a plateau-like pattern on pupillographic recordings. It reflects delayed transition from parasympathetic to sympathetic dominance, resulting in a “frozen” pupil following light-induced constriction. The condition is commonly observed in chronic alcoholism and is attributed to weakened cholinergic mechanisms and reduced parasympathetic tone.
Cheyne–Stokes Respiratory Pupillary Response
Pupillary reactions are absent during apneic phases, exhibit progressive dilation during forced inspiration, and rapidly return to baseline as respiratory depth decreases.
Accommodation Reflex
Pupillary constriction occurs during fixation on near objects and dilation during distance viewing, accompanied by ocular convergence.
Convergence Reflex
Pupillary constriction accompanies medial eye movement during convergence, reaching maximal adduction when the target is approximately 10–15 cm from the eyes.
Pain-Induced Pupillary Reflex
Noxious stimulation produces pupillary dilation mediated by subthalamic reflex centers that activate the pupillary dilator musculature.
Trigeminal Pupillary Reflex
Stimulation of the cornea, conjunctiva, or periocular tissues induces initial pupillary dilation followed by constriction, mediated through trigeminal afferents and subcortical sympathetic pathways.
Galvanic Pupillary Reflex
Application of galvanic current—with the anode placed over the eye or temporal region and the cathode over the posterior cervical region—elicits pupillary constriction.
Cochleo-Pupillary Reflex
Bilateral pupillary dilation occurs in response to vestibular stimulation, such as rotational movement.
Pharyngeal Pupillary Reflex
Irritation of the posterior pharyngeal wall results in pupillary dilation mediated via glossopharyngeal and superior laryngeal nerve pathways.
Cortically Mediated Imagery-Induced Pupillary Responses
Imagined darkness may elicit pupillary dilation (Piltz phenomenon), whereas imagined bright light may induce constriction (Gaab phenomenon), reflecting higher cortical modulation of pupillary function.